The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.
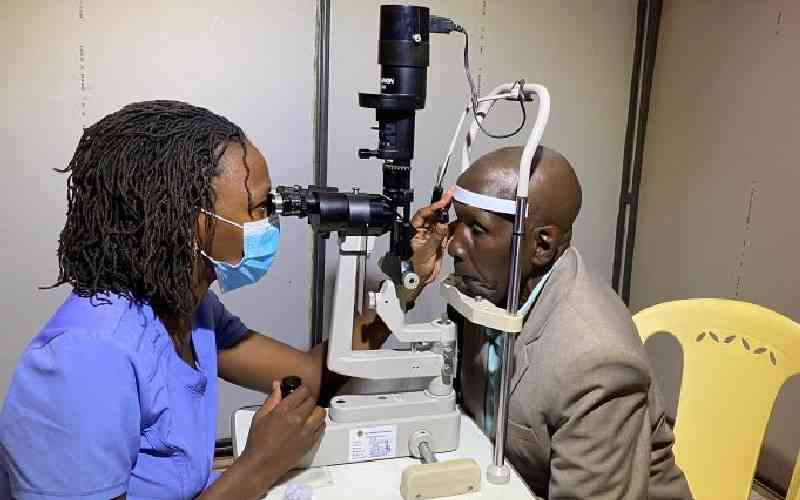
Dr Lily Nyamai Adhiambo an Ophthalmologist and Glaucoma specialist, conducts eyecheck up on Jimna Waweru during a free glaucoma medical camp at Lions SightFirst Eye Hospital in Loresho, Nairobi. [File, Standard]
New data from the International Agency for the Prevention of Blindness (IAPB) and the Seva Foundation shows that the right pair of glasses can help a child learn and earn more. Every school year, Kenya loses 24,959 years of potential learning because the children in class can’t see properly. We are talking about uncorrected refractive error with an estimated 86,000 children and adolescents having vision problems such as short-sightedness and long-sightedness. According to the IAPB, the burden of poor eye health to the economy is estimated to be Sh14.8 billion every year in unrealised economic potential, pointing to the need for heightened nationwide preventive and curative programmes.
This year’s World Sight Day, focusing on child eye health, reminds us that we have a long way to go in the journey to reducing national incidences of poor vision and facilitating citizens with sight challenges to become economically productive. In jurisdictions like Kenya and India, regular preventive measures such as screening programmes that facilitate early detection are being established in schools for children between five and 15-years-old. These programmes' success, however, hinges on key factors including the availability of trained teachers, access and affordability, parental awareness and a community-led health system that tracks the child’s progress.
One documented case study of the LV Prasad Eye Institute in India set out to provide eye screening to children aged between 0 and 15 in schools and villages in Krishna District. It started by obtaining approvals from the appropriate local government authorities, training selected nominated teachers, pre-screening the children at school and allocating community health workers to follow up with those referred to local hospitals for further treatment.
The experience showed that in addition to alerting the village elders, in most schools only one teacher was nominated to be trained by an experienced eye care professional. The training content included structure and functions of the eye, refractive errors, common eye conditions in children and vision screening procedures to diagnose and correct them. The programme also trained specific Community Eye Health Workers (CEHW) to work alongside the teachers.
Arming the CEHW with such specific knowledge and skills was a game-changer in promoting preventive and curative awareness. In addition to referring children identified with eye challenges to a primary eye care centre close by, a full-time CEHW along with a coordinator was assigned to follow up on these individual cases. Uptake of the eye care solutions such as using recommended spectacles was considered a key success area.
To achieve a high uptake of up to 90 per cent, the eye care professional examined children in schools and involved parents through group meetings, including calling those who did not turn up and providing travel to the ones who were unable to afford it. Ultimately, considerable time and effort were required to counsel and convince parents and caregivers to bring the children to access eye care services.
With Kenya’s Community Health Promoter (CHP) programme in place, I see an opportunity to emulate the Krishna case through the Primary Care Networks (PCN) being rolled out across the country. This is because they are trained to work as a link between the community and formal health facilities.
They are at the forefront of disseminating vital information on nutrition, hygiene, and disease prevention. By addressing health challenges at their roots, these promoters contribute significantly to reducing the burden on the healthcare system and enhancing the overall quality of care. Importantly, this model recognises the critical need for robust referral pathways.
In addition to setting up nearly 200 PCNs, the Kenyan government has deployed over 100,000 Community Health Promoters (CHPs) across the 47 counties. As Kenya’s pursuit of Universal Health Coverage (UHC) by 2030 highlights the necessity of integrating eye health into mainstream primary care, a lack of eye health knowledge among CHP will be a major hurdle. This is further compounded by the limited number of trained eye care service providers and the concentration of eye care services in referral hospitals, leading to overcrowding and extended waiting times.
The steep cost of eye care services also hinders accessibility for economically disadvantaged individuals especially those in low-income households. Unfortunately, evidence shows that while young children are most at risk of intensified complications and avoidable blindness, addressing poor vision early unlocks an extra Sh2 million in individual lifetime earnings.
Addressing these challenges comprehensively requires a multifaceted approach comprising eye health awareness and services, comprehensive training for CHPs, actively championing eye health in local barazas, and advocating to disseminate knowledge, challenge stigma to dispel myths surrounding eye problems and spectacles.
It also calls for training multiple teachers in each school environment with basic eye health assessment skills and working with them as local champions. We have much to gain by fixing the system for our children, including ensuring they have the right pair of glasses to enable them learn and earn more as economically productive adults.
 The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.
The Standard Group Plc is a
multi-media organization with investments in media platforms spanning newspaper
print operations, television, radio broadcasting, digital and online services. The
Standard Group is recognized as a leading multi-media house in Kenya with a key
influence in matters of national and international interest.